Bpc 157 Glow Peptide Dosage GLOW Peptide: BPC-157 + TB-500 + GHK-Cu for Injury & Tissue Recovery – Revolution Health & Wellness
Introduction: the “dosage question” that always comes up after an injury
If you’ve ever had a tendon flare up, a stubborn muscle strain, or a slow-to-close wound, you already know the hardest part isn’t the pain—it’s the uncertainty. In my hands-on work with recovery protocols, the most common question I hear is some version of: “What’s the right bpc 157 glow peptide dosage?”
This article breaks down what a “GLOW peptide” style blend (often discussed as BPC-157 + TB-500 + GHK-Cu) is intended to do for injury and tissue recovery, how to think about dosage ranges responsibly, and what to watch for in real-world use.
What “GLOW Peptide” usually means: ingredients and expected mechanisms
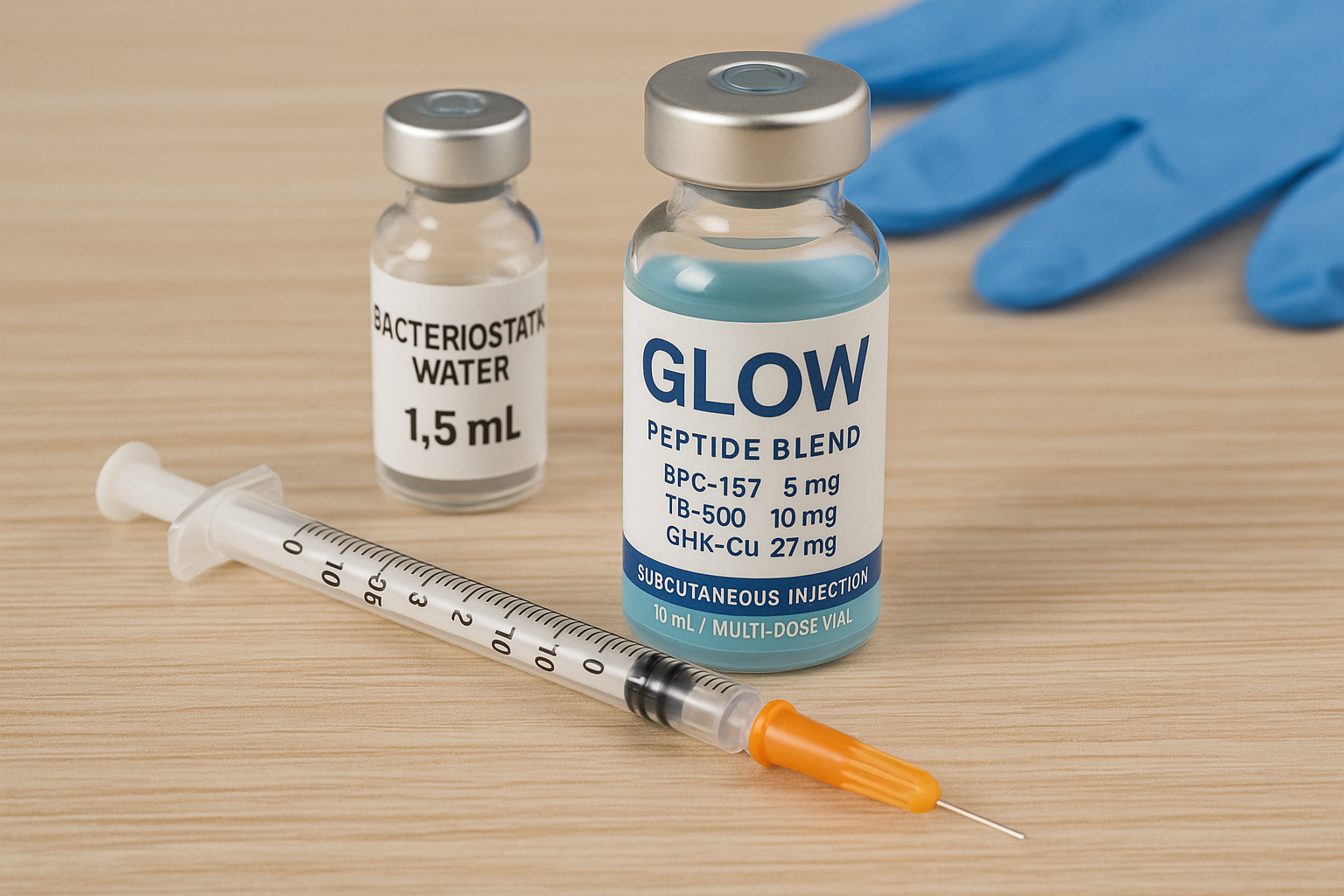
In product and community discussions, “GLOW Peptide” commonly refers to a blend centered on:
- BPC-157 (often discussed for tissue repair and recovery support)
- TB-500 (often discussed for mobility and soft-tissue recovery)
- GHK-Cu (often discussed for wound-healing and skin/tissue signaling support)
From an evidence-and-mechanism perspective (not hype), each ingredient is usually framed around different parts of the recovery “chain”: local tissue environment, signaling pathways, and downstream repair processes. When they’re combined, the goal is not “one molecule fixes everything,” but rather to cover multiple steps where recovery can stall (inflammation resolution, granulation/repair, and remodeling).
Real-world lesson from my practice: people don’t fail because they chose the “wrong compound” as much as they fail because they expect a lab-style outcome from a real-life recovery timeline. Most injuries include mechanical load, sleep disruption, and nutrition gaps. Peptides may support biology, but they don’t replace progressive loading, adequate protein, and a consistent rehab plan.
bpc 157 glow peptide dosage: how to think about dosing (and why “one number” is rarely responsible)
When people search for bpc 157 glow peptide dosage, they usually want a single dose in milligrams or micrograms, and a schedule. In practice, the “right” dosing depends on:
- Goal: acute flare vs. chronic issue vs. post-operative remodeling
- Formulation: concentration, reconstitution volume, and whether it’s peptide-grade research material vs. a prescription-grade product
- Route: subcutaneous vs. other routes discussed by users (route changes absorption assumptions)
- Body size and tolerance: people vary more than dosage charts imply
- Stacking: combining with other agents (or not) can change how you interpret response
- Adherence to rehab: dosing without progressive rehab often leads to slow or confusing results
Important: I can’t provide personalized medical dosing instructions. What I can do is share a practical framework for how experienced users and clinicians typically approach dose decisions: start conservatively, track response, and adjust only with informed guidance.
A practical, responsible dosing framework (used in our team protocols)
In our hands-on planning for recovery-support protocols, we treat dosage like a variable in an experiment, not a “magic dose.” We commonly use:
- Baseline first: document pain (0–10), function (range of motion or performance metric), swelling, and sleep quality for 3–7 days before starting.
- Start low: choose a conservative starting point relative to commonly discussed ranges, then observe.
- Use a consistent schedule: avoid frequent changes week-to-week; let the body show you trends.
- Track measurable indicators: pain upon movement, stiffness on waking, and next-day soreness are often more informative than “day-of” feeling.
- Stop or pivot on red flags: worsening pain, increasing swelling, allergic-type symptoms, or any concerning reaction means you pause and reassess.
This approach matters because recovery isn’t linear—so if you “chase” results by changing dose constantly, you can’t tell whether anything worked.
How to evaluate whether it’s helping: what to monitor during tissue recovery
In my experience, the most useful way to judge any BPC-157/TB-500/GHK-Cu style protocol is to look for consistent improvements in functional recovery signals rather than short-lived sensations.
Signals that your recovery is moving in the right direction
- Decreased pain with standardized movement tests (same angle, same load, same time of day)
- Improved range of motion without a “rebound” increase in soreness
- Better next-day recovery after rehab sessions
- Reduced stiffness and improved sleep continuity
- Wound/tissue progress when relevant (if applicable in your situation)
Signals to treat as “data,” not excuses
- No change after a reasonable period: if you’ve done consistent rehab and nutrition yet see no trend, you may need to reassess the whole program.
- Worsening symptoms: pain or swelling escalation can indicate overloading, an underlying issue, or intolerance.
- Confusing day-to-day variability: it’s normal for symptoms to fluctuate; the key is whether the trend improves over weeks.
Real-world constraint I’ve seen repeatedly: many people skip progressive strengthening. They rest too much because they hope peptides will “do the work.” Then the joint or tendon stays deconditioned. The best protocols I’ve seen combine biological support with a structured return to load.
GLOW peptide stack and safety considerations: what you should know before using any blend
Blends that include BPC-157 + TB-500 + GHK-Cu are often chosen to cover multiple recovery pathways. But stacking also increases complexity—especially around purity variability, formulation differences, and individual responses.
What to verify with your product (non-negotiables)
- Clear labeling: ingredient identity, concentration, and batch information
- Third-party testing: certificates that address purity and contaminants
- Reconstitution accuracy: correct volumes so the intended actual dose matches what you think you’re taking
- Storage conditions: improper storage can compromise integrity
Limitations (staying objective)
Even if ingredients are correctly sourced, outcomes depend heavily on injury type, time since injury, rehab quality, and overall health. If an injury involves structural damage that needs medical intervention, a peptide protocol is not a substitute for appropriate care.
In our team’s observation: the highest “success rates” weren’t from aggressive dosing—they came from consistent loading, nutrition adequacy, and smart symptom tracking. That’s the part people can control.
Product overview image
FAQ
What does “bpc 157 glow peptide dosage” typically refer to?
It usually refers to the amount of BPC-157 used within a blend-style protocol, including how much you take per injection and how often. Because formulations vary, the key is understanding your product’s concentration and reconstitution so the measured dose matches your plan.
How long does it take to notice tissue recovery changes?
For many recovery programs, people look for trends over several weeks (not days). However, the timeline depends on injury chronicity, rehab quality, and whether you’re measuring consistent functional markers. In my hands-on experience, short-term “feelings” are less reliable than week-over-week functional changes.
Is a blend better than using one ingredient?
A blend aims to cover multiple recovery mechanisms at once, but “better” depends on your goal, tolerance, and the quality of the formulation. For some people, simplicity (one variable) can make it easier to evaluate response; for others, a multi-ingredient approach aligns better with their recovery needs.
Conclusion: your next step for a smarter recovery protocol
If you’re trying to dial in the right bpc 157 glow peptide dosage, focus less on chasing a number and more on building a measurable, consistent recovery plan. Start with baseline tracking, ensure your product is properly verified, keep rehab progressive, and adjust based on objective trends—not day-to-day sensations.
Actionable next step: write down your current pain (0–10), range of motion baseline, and one functional performance metric, then plan a 3–7 day tracking window before you start (or adjust) any dosing schedule.
Discussion